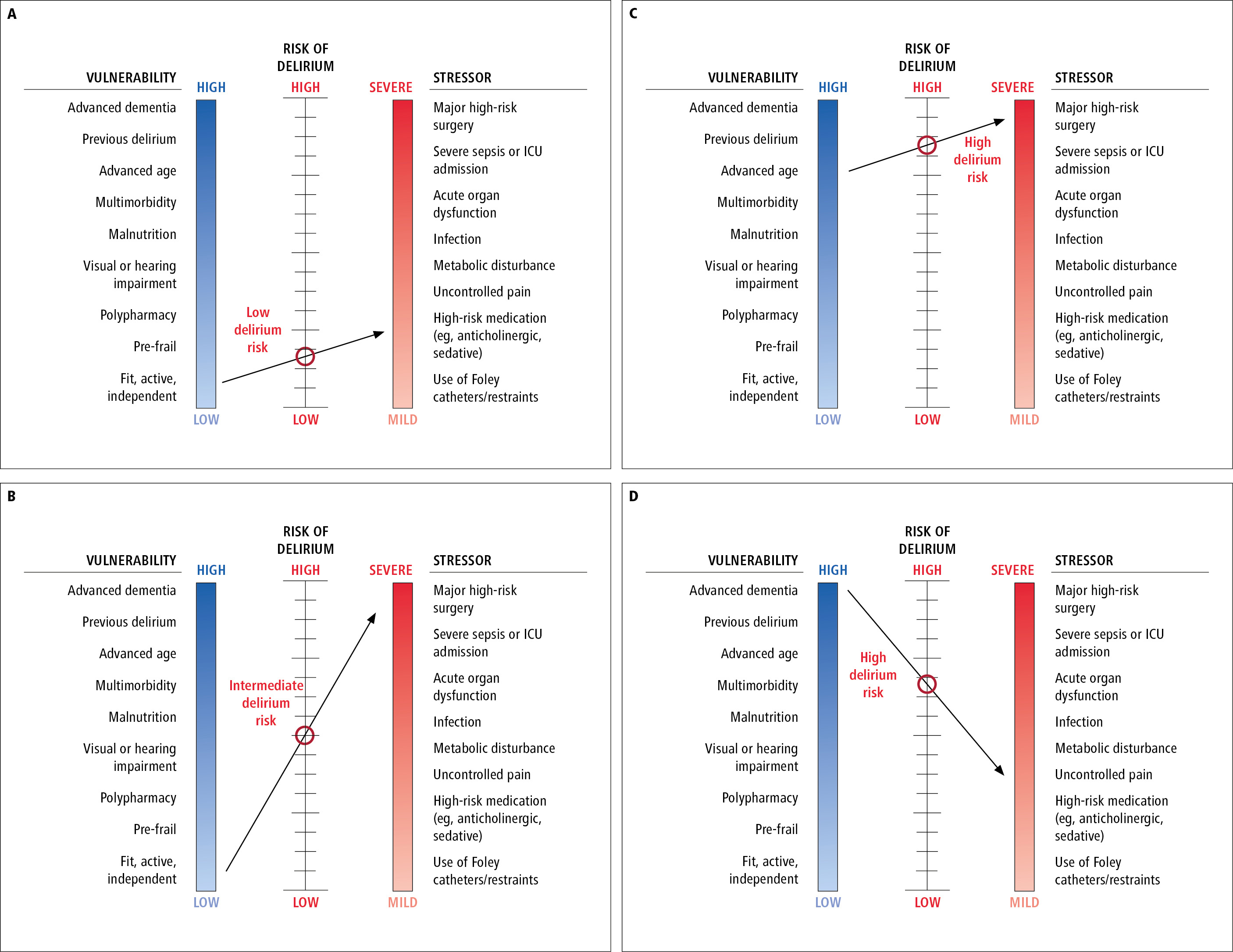
Four scenarios illustrating interactions between vulnerability, stressor, and delirium risk. A line connecting the perceived vulnerability and stress levels determines the point of intersection on the delirium risk scale. Scenario A, an older adult that is fit, active, and independent with activities of daily living (low vulnerability) is prescribed a daily benzodiazepine for primary insomnia (mild stressor). The risk for developing delirium with short-term or long-term use of this high-risk drug is anticipated to be low. Scenario B, an older adult that is fit, active, and independent with activities of daily living (low vulnerability) is scheduled for coronary artery bypass grafting (severe stressor). The risk for developing postoperative delirium is anticipated to be intermediate. Scenario C, a frail 95-year-old adult with multimorbidity (high vulnerability) is scheduled for coronary artery bypass grafting (severe stressor). The risk for developing postoperative delirium is anticipated to be very high. Scenario D, an older adult with advanced dementia who is dependent for all activities of daily living (high vulnerability) is prescribed a daily benzodiazepine for primary insomnia (mild stressor). The risk for developing postoperative delirium is anticipated to be very high. Inspired by JAMA. 1996;275(11):852-7.