A 75-year-old female patient who presented with exertional dyspnea. You order a chest x-ray (Fig. 1a, b).
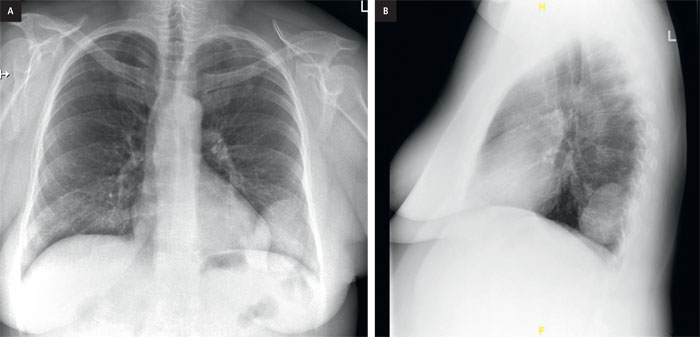
Figure 1. PA (a) and lateral chest x-ray (b).
Do you see an abnormality on the PA and lateral views?
If you do not see an abnormality on PA or lateral chest x-rays, take the systematic approach to interpretation. A full review of the systematic approach is found in "Discover Radiology: Chest x-ray interpretation" book, Chapter 5 (An Introduction to chest x-ray interpretation).
The x-ray shows a large well-circumscribed, non-calcified mass (Fig. 2a) overlying the inferior left side of the chest. There are tubular elongated structures that appear to emulate from the mass coursing towards the left hilum. On first glance you may think that this mass is associated with the left breast. However, when you look on the lateral x-ray (Fig. 2b) you can see that this mass (arrows) lies posterior and by process of elimination can only lie within the left lung.
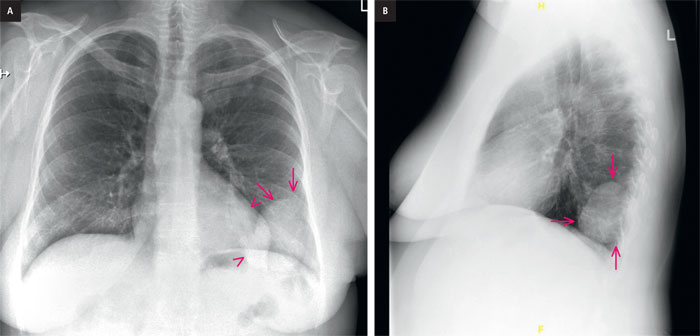
Figure 2. a, PA chest x-ray. A well-circumscribed, non-calcified mass (arrow) lies within the left lung.
Tubular elongated structures (arrowheads) are seen extending from the mass coursing towards the left hilum, b, lateral Chest X-ray. A well-circumscribed, non-calcified mass (arrows) lies posteriorly within
the left lung.
To further characterize the abnormality a Chest CT scan was performed (Fig. 3).
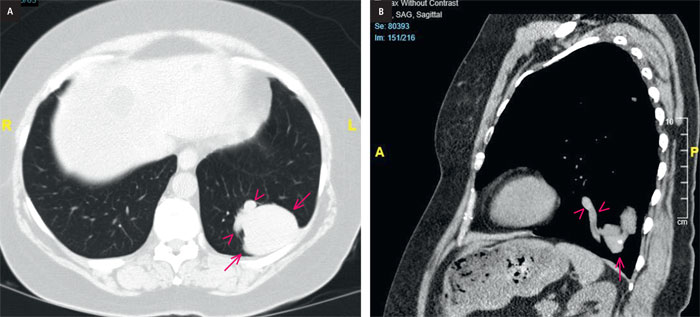
Figure 3. a, axial CT scan. A well-circumscribed, non-calcified mass (arrows) is confirmed within the left lung.
Tubular elongated structures (arrowheads) are seen extending from the mass, b, sagittal CT scan. Tubular elongated structures (arrowheads) are seen extending from the mass (arrows).
Note the presence of a small focal area of calcification within the mass (phlebolith).
Summary
The CXR and CT scan showed a smooth, well defined lesion in the left lower lobe, with pulmonary arterial branches extending into the lesion and pulmonary veins extending out of the lesion.Diagnosis
Pulmonary arteriovenous malformation (PAVM)
This was successfully treated by pulmonary angiogram (Fig. 4a, b) and embolization with coils (Fig. 4c) by interventional radiology. The follow-up chest x-ray (Fig. 5) and CT scan show complete resolution of the PAVM. The patients symptoms were completely resolved a few weeks after the procedure.

Figure 4. Pulmonary angiogram. a, pulmonary artery injection of contrast shows blood vessels (arrows)
leading into a large blood-filled space (arrowheads). Delayed images show large veins (arrow) draining from the
lesion into the left hilum, c, post-embolization images show coils (arrows) within the arterial portion of the
pulmonary arteriovenous malformation.
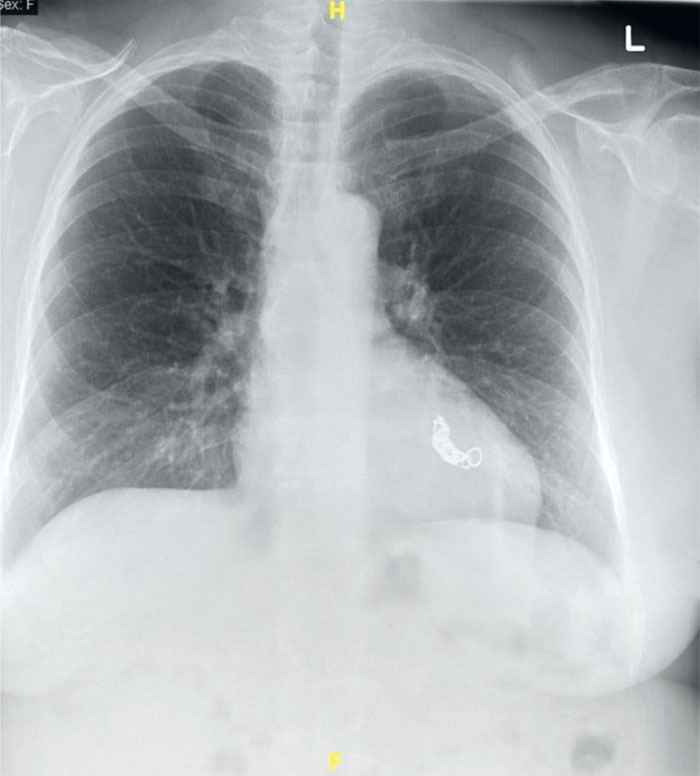
Figure 5. PA chest x-ray. The follow-up post-embolization chest x-ray shows complete resolution
of the PAVM.
You can find more interesting cases in the app "Discover Radiology: Chest x-ray interpretation".
Price – only $6.99
References
Hsu CC, Kwan GN, Evans-Barns H, van Driel ML. Embolisation for pulmonary arteriovenous malformation. Cochrane Database Syst Rev. 2018 Jan 4;1(1):CD008017. doi: 10.1002/14651858.CD008017.pub5. PMID: 29298459; PMCID: PMC6491094.Tellapuri S, Park HS, Kalva SP. Pulmonary arteriovenous malformations. Int J Cardiovasc Imaging. 2019 Aug;35(8):1421-1428. doi: 10.1007/s10554-018-1479-x. Epub 2018 Nov 1. PMID: 30386957.