You order a chest x-ray and PA and lateral views are obtained (Fig. 1a,b).
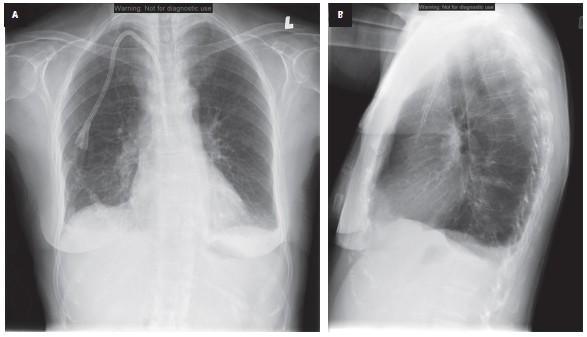
Figure 1. a, PA chest x-ray, b, lateral chest x-ray.
Question
Can you identify a major abnormality on the PA view and on the lateral view?
Compare to a normal PA and lateral chest x-ray (Fig. 2A,B)
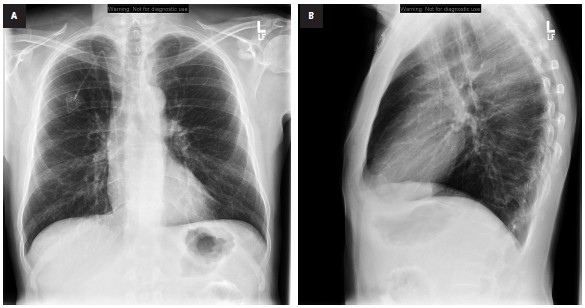
Figure 2. The example of normal PA and lateral chest x-ray.
If you identified the abnormality on the PA or lateral, or both, your interpretation is still not complete.
You now need to review all the other anatomical structures to make sure nothing else is wrong.
If you did not identify the abnormality you will need to do a systematic review of the chest x-ray.
My approach is to systematically evaluate the chest x-ray in the following 7 steps:
- Trachea and bronchi
- Heart
- Mediastinum
- Hila
- Lungs
- Pleura
- Chest wall
How should the position of the central venous catheters (CVCs)look like?
Radiological anatomy of the superior vena cava (SVC)
On the PA x-ray, the SVC (together with the right brachiocephalic vein) forms the right superior edge of the mediastinum (Fig. 3).
This edge extends vertically from the right heart border superiorly, into the thoracic inlet (Fig. 4a,b).
From the lateral perspective, the SVC descends from the thoracic outlet superiorly, lying anterior to the trachea and the right pulmonary artery (RPA), and eventually drains into the right atrium (Fig. 4c).
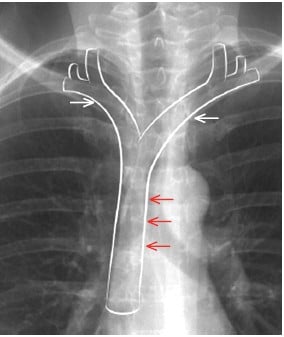
Figure 3. Radiological anatomy of the superior vena cava (SVC; red arrows) and brachiocephalic veins(white arrows).
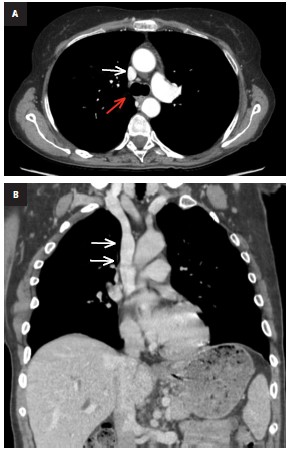
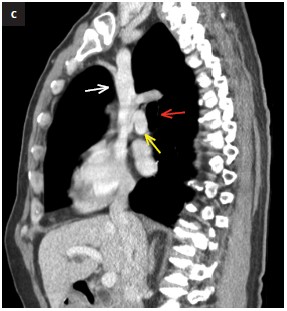
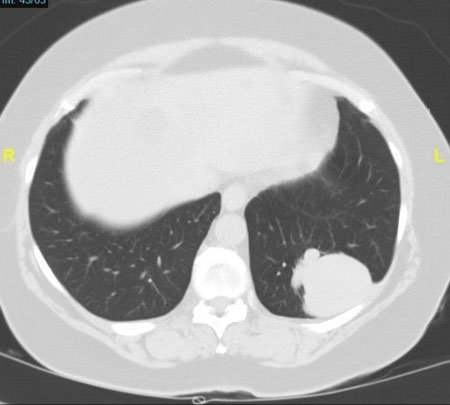
Figure 4. The superior vena cava (white arrows) in the computed tomography scan (CT). a, cross-sectional imaging (right main stem bronchus at the level of the carina – red arrow ), b, coronal plane. c, sagittal plane(anterior wall of trachea – red arrow, left pulmonary artery – yellow arrow.
Because of this positioning, the SVC is not seen as a distinct structure on the lateral x-ray. Normally, the SVC forms a straight vertical edge on the PA x-ray; suspect pathology if this edge is bulging outward (Fig. 5.).
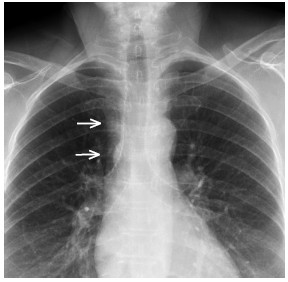
Figure 5. The superior vena cava forms a straight vertical edge (arrows).
Findings in this case
The position or course of the CVCs is different than expected. On the PA chest x‑ray (Fig. 1a) the
catheter is more medial than expected.
Then, when we look on the lateral (Fig. 1b) instead of being positioned just anterior to the trachea the catheter courses anterior
and inferior. Wow! The only anatomical position possible for the catheter is the thoracic aorta, and this was confirmed with a CT scan.
Diagnosis
Aberrant CVP in the thoracic aorta
You can find more interesting cases in the app "Discover Radiology: Chest x-ray interpretation".
Price – only $6.99