A 63-year-old male patient is seen in your office with a persistent cough. He believes the coughing started after eating chicken.
You order a chest x-ray and PA and lateral views are obtained (Fig. 1a,b).


Figure 1. a, PA chest x-ray, b, lateral chest x-ray.
Questions
Can you identify an abnormality on the PA and on the lateral views?
If you identified the abnormality on the PA, on the lateral or on both projections, your interpretation is still not complete.
You now need to review all the other anatomical structures to make sure nothing else is wrong. To identify the abnormality, you will need to do a systematic review of the
chest x-ray. My approach is to systematically evaluate the chest x-ray in the following 7 steps:
- Trachea and bronchi
- Heart
- Mediastinum
- Hila
- Lungs
- Pleura
- Chest wall
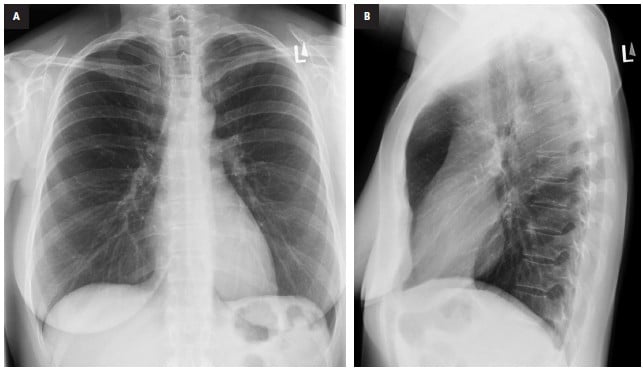
Figure 2. Normal chest x-ray. a, PA chest x-ray, b, lateral chest x-ray.
- While doing a systematic evaluation of Fig 1a and 1b you may be curious if something is wrong behind the heart on the left. You would be correct.
- What should this area look like on a chest x‑ray?
- What should a normal retrocardiac region look like on the x‑ray?
Relevant anatomy and radiological anatomy
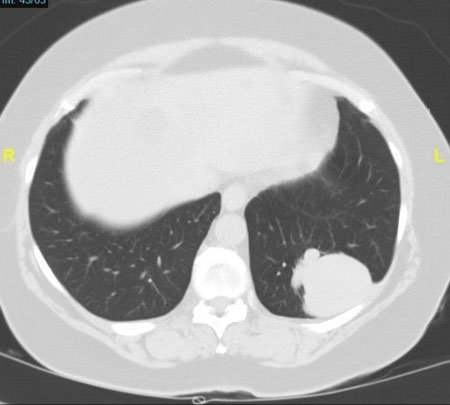
Directly behind the heart lies the left lung. The descending branch of the left pulmonary artery is frequently seen through the heart. Otherwise this region has a fairly homogeneous density (Fig. 3a,b).
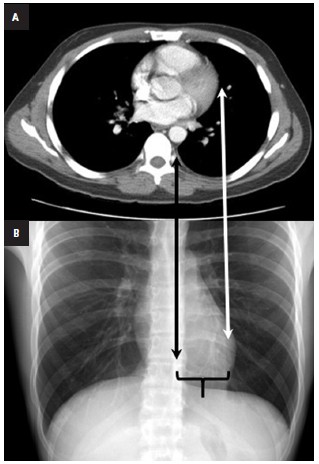
Figure 3. a, axial CT through chest at level of the heart, b,correlation of the PA chest x-ray. The white arrow points to
the interface between the lung and the most lateral aspect of the heart. The black arrow points to the interface between the lung and the most
lateral aspect of the heart. Note the normal density of the retrosternal airspace (between the two arrows).
Findings in case
Now, if we look at our case again (Fig. 1a) and compare it with a normal example (Fig. 2A), we can confidently see the space behind the heart is too white. There is a triangular shaped density with a smooth upper border. The lateral projection (Fig 1b) looks completely normal (compare with normal lateral example; Fig. 2b).
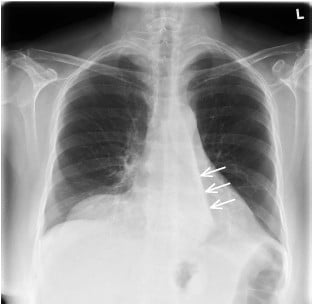
Figure 4. The smooth edge of the retrocardiac density is highlighted with white arrows on the PA.
Summary
Homogeneous triangular density in the retrocardiac region.What can cause a homogeneous triangular density in the retrocardiac region?
The important finding in this case is the smooth upper edge of the triangular density. When I identify a smooth flat edge on a chest x-ray, I immediately consider that the edge is caused by a pleural fissure and that the adjacent increased density is caused by non opacified lung. In our case the edge is too inferior compared to an expected normal position.
Diagnosis
The only explanation for the findings is collapse of the left lower lobe.
Discussion: On the PA image the left oblique fissure (which divided the left upper lobe from the left lower lobe) is usually not visible (Fig 5a). When there is volume loss within the left lower lobe the density of the left lower lobe starts to increase and the lower lobe with a smooth edge (the fissure) starts to be visible (Fig. 5b). The direction of the left lower lobe collapse is posterior, inferior and medial. With further collapse the left lower lobe becomes more homogeneously dense and forms the triangular density behind the heart (Fig. 5c).
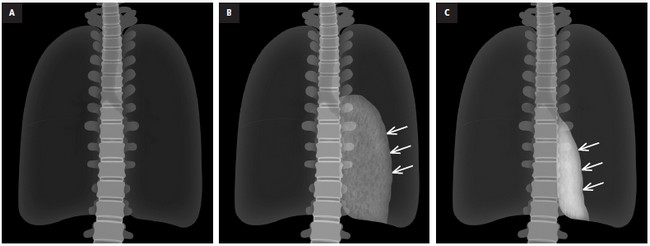
Figure 5. a, illustration showing normal lungs. The oblique fissure is usually not visible, b, when there is volume loss within the left lower lobe the density of the left lower lobe starts to increase and the lower lobe with a smooth upper edge (the fissure) starts to be visible. The left lower lobe shiftsinferior (white arrows), c, with further collapse the left lower lobe positions posterior, inferior and medially (white arrows) and creates the appearance of a triangle in the retrocardiac region.
Radiological Signs/Features of Lobar Collapse
The radiological signs/features of lobar collapse can be divided into direct and indirect.
Direct sign of collapse
The hallmark, and only direct sign, of collapse is the shift of the fissures.
Indirect signs of collapse
- Increased lung opacity
- Compensatory hyperinflation of the surrounding lung
- Obscured cardiac, mediastinal, or diaphragmatic borders
- Crowding of pulmonary vessels
- Elevated diaphragm
- Hilar displacement
- Crowding of the ribs
You can find more interesting cases in the app "Discover Radiology: Chest x-ray interpretation".
Price – only $6.99