 English
English
 Español
Español
 українська
українська

Baumgartner H, De Backer J, Babu-Narayan SV, et al; ESC Scientific Document Group. 2020 ESC Guidelines for the management of adult congenital heart disease. Eur Heart J. 2021 Feb 11;42(6):563-645. doi: 10.1093/eurheartj/ehaa554. PMID: 32860028.
Stout KK, Daniels CJ, Aboulhosn JA, et al. 2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019 Apr 2;139(14):e637-e697. doi:10.1161/CIR.0000000000000602. PMID: 30586768.
Definition and Clinical FeaturesTop
Ebstein anomaly is a congenital malformation of the tricuspid valve resulting in failure of delamination during cardiac development. This congenital anomaly may remain undiagnosed until adulthood. It includes a wide range of lesions, which depend on the degree of displacement of the septal tricuspid leaflet into the right ventricle, “atrialization” of the right ventricle, severity of functional changes (regurgitation or stenosis of the tricuspid valve), coexisting interatrial shunt (patent foramen ovale or atrial septal defects in 50%-75% of patients), accessory conduction pathways (usually right-sided, may be multiple), and other coexisting congenital malformations. Although mild forms of Ebstein anomaly may be asymptomatic, severe forms may cause a significant reduction in exercise tolerance. Accessory pathways (often multiple), which may be concealed, are commonly present.
Symptoms: Palpitations, dyspnea, reduced exercise tolerance, often mild cyanosis. Patients with mild defects are usually asymptomatic until a late age; in others, symptoms develop in the second and third decades of life.
Signs: On auscultation, midsystolic heart sounds (clicks, often multiple), a holosystolic murmur that intensifies during inspiration (this is caused by tricuspid regurgitation), wide splitting of the first and second heart sounds, and a right ventricular third heart sound.
Diagnosis Top
Diagnosis is usually based on echocardiography with evidence of apical displacement of septal and posterior leaflets of the tricuspid valve.
1. Electrocardiography (ECG): Right atrial enlargement (very tall P waves, >5 mm) and splintered multiphasic right bundle branch block–like QRS complexes are typically seen. ECG should be inspected for the presence of preexcitation (right-sided bypass tract).
2. Chest radiography may be nearly normal in mild cases and show severe enlargement (globular or box shaped) of the right atrium in severe cases. The lungs and pulmonary vasculature appear normal in mild cases and oligemic in severe cases.
3. Echocardiography (Figure 1): Apical displacement of septal and posterior leaflets of the tricuspid valve (for septal leaflets, ≥0.8 cm/m2). There are varying degrees of tricuspid regurgitation. The presence of an atrial-level shunt should be documented; this is usually best achieved with intravenous bubble contrast injection during echocardiography.
4. Magnetic resonance imaging (MRI): Preoperative evaluation may be warranted to provide a complete anatomical assessment. Accurate volumetric evaluation of the right ventricle can be obtained with MRI.
Treatment Top
Surgery is indicated in patients with New York Heart Association (NYHA) class III or higher, cyanosis, right ventricular heart failure, or paradoxical embolism. Relative indications include recurrent supraventricular arrhythmias resistant to treatment (including ineffective ablation) and significant asymptomatic heart enlargement. Surgery should be performed by surgeons with special expertise in operating on adults with congenital heart disease as well as special expertise in different techniques used in surgical repairs in patients with Ebstein anomaly. Surgical treatment improves prognosis. Continuing periodic follow-up in specialized clinics postoperatively is recommended.
FiguresTop
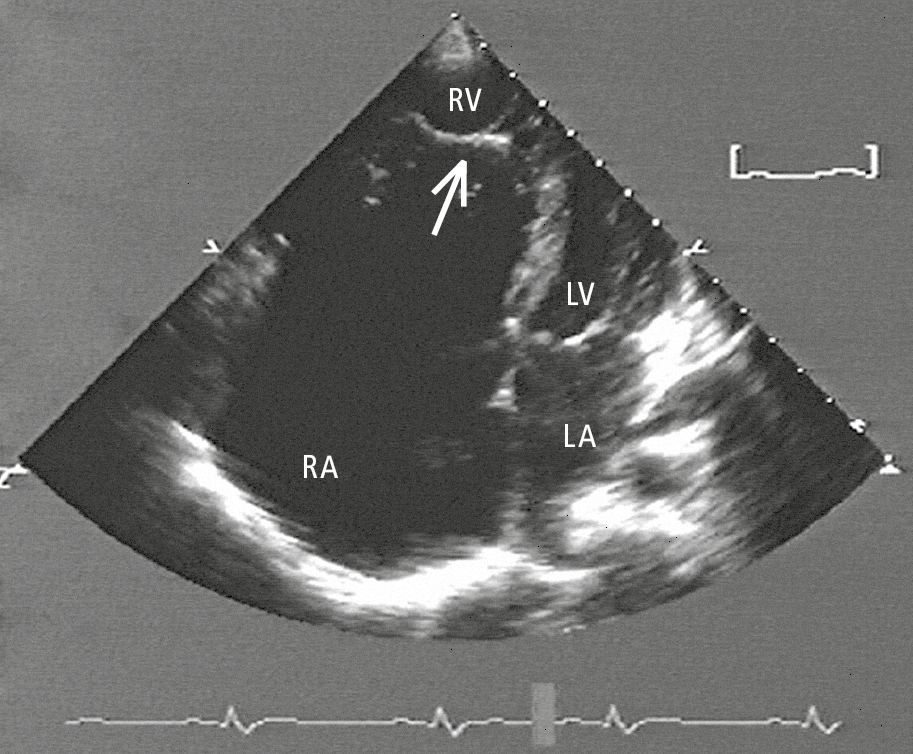
Figure 3.7-1. Transthoracic echocardiography (TTE) of a patient with Ebstein anomaly: significant displacement of the septal leaflet into the right ventricle (arrow). LA, left atrium; RA, right atrium; RV, right ventricle.