 English
English
 Español
Español
 українська
українська

Rihal, CS, Naidu SS, Givertz MM, et al. 2015 SCAI/ACC/HFSA/STS Clinical Expert Consensus Statement on the Use of Percutaneous Mechanical Circulatory Support Devices in Cardiovascular Care. JACC. 2015 May 65(19):e7-26. doi: http://dx.doi.org/10.1016/j.jacc.2015.03.036. PMID: 25861963.
Unverzagt S, Buerke M, de Waha A, et al. Intra‐aortic balloon pump counterpulsation (IABP) for myocardial infarction complicated by cardiogenic shock. Cochrane Database of Systematic Reviews 2015, Issue 3. Art. No.: CD007398. doi: 10.1002/14651858.CD007398.pub3. PMID: 25812932; PMCID: PMC8454261.
The intra-aortic balloon pump (IABP) is used to improve oxygen delivery to the myocardium; the improvement in peripheral perfusion is usually insignificant. The operation of an IABP (Figure 21.10-1) involves inflation and deflation of a 30- to 50-mL balloon, inserted through the common femoral artery into the descending aorta distal to the exit of the left subclavian artery, that is synchronized with cardiac function monitored by electrocardiography (ECG) or a blood pressure curve. An IABP can be introduced percutaneously or surgically through the femoral artery, and in the case of advanced atherosclerosis of the arteries of the lower extremities, through another vessel (eg, aorta).
Key hemodynamic effects of an IABP:
1) Transport of blood to the proximal aorta by inflating the balloon during diastole, which improves coronary artery blood flow and thus myocardial perfusion.
2) Afterload reduction through rapid deflation of the balloon creates a vacuum effect during systole and reduces myocardial oxygen consumption.
An optimal hemodynamic benefit depends on the balloon volume and position; timing of the balloon inflation in diastole and deflation during systole; and patient’s own cardiac function, heart rate, blood pressure, aortic compliance, and vascular resistance.
IndicationsTop
1. As a bridge to recovery (BTR), bridge to decision (BTD), or bridge to bridge (BTB) in cardiogenic shock, including treatment of the underlying cause of cardiogenic shock (eg, mechanical complications of acute myocardial infarction).
2. Low cardiac output syndrome following cardiac surgery.
3. High-risk percutaneous coronary intervention (PCI).
Based on the IABP-SHOCK II randomized trial and a Cochrane review of 7 trials, IABPs may have a beneficial effect on some hemodynamic parameters, but their use does not result in short-term or long-term survival benefits. Therefore, IABPs are not routinely recommended in cardiogenic shock but should be considered in acute coronary syndrome (ACS)–related mechanical complications such as acute mitral regurgitation, ventricular septal defects, or left ventricular failure.
ContraindicationsTop
Aortic regurgitation, aortic dissection, advanced atherosclerosis in the lower extremities and aorta.
ComplicationsTop
Vascular (9%-25% of patients): Lower limb ischemia (much less often: visceral or spinal cord ischemia), damage to the vessel wall (aortic dissection requires immediate balloon removal), and severe bleeding.
Extravascular: Sepsis, hemolysis, thrombocytopenia, peripheral neuropathy, balloon rupture, death (<2%).
FigureSTop
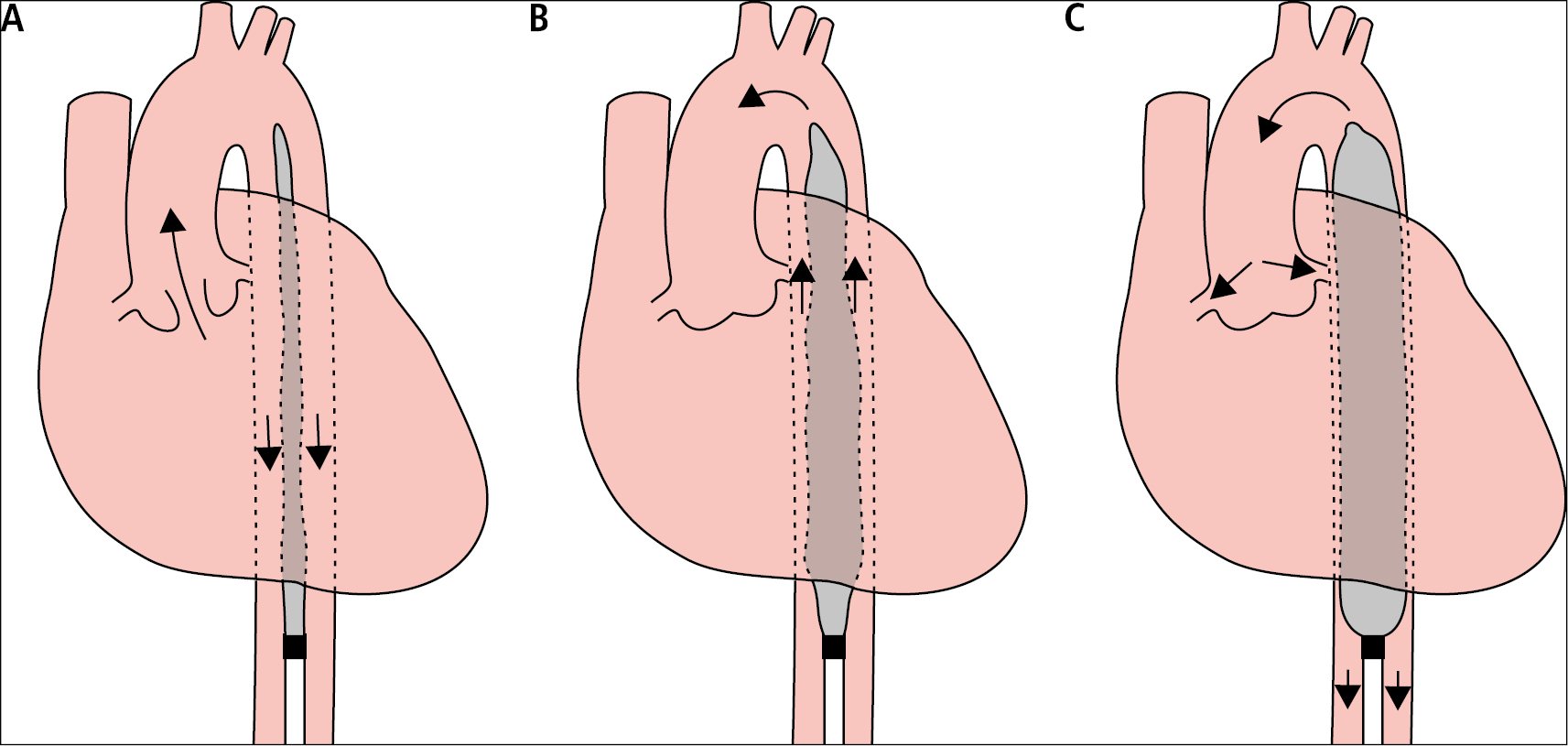
Figure 21.10-1. The operating principle of an intra-aortic balloon pump (IABP). A, contraction of the heart, balloon deflated. B, early heart diastole, starting balloon inflation. C, late diastolic phase, complete balloon inflation.