 English
English
 Español
Español
 українська
українська

Clark AL, Cleland JG. Causes and treatment of oedema in patients with heart failure. Nat Rev Cardiol. 2013 Mar;10(3):156-70. doi: 10.1038/nrcardio.2012.191. Epub 2013 Jan 15. Review. PubMed PMID: 23319101.
Definition and PathogenesisTop
Edema (swelling) is the accumulation of fluid in the tissue interstitium.
1. Mechanism: There are 4 major mechanisms that fundamentally lead to edema. Frequently ≥1 mechanism is present:
1) Increased hydrostatic pressure at the venous end of the capillary bed (eg, in patients with congestive heart failure [HF] or venous valve incompetence).
2) Decreased plasma oncotic pressure (due to hypoalbuminemia).
3) Increased capillary wall permeability (most frequently due to inflammation).
4) Impaired lymphatic drainage (eg, in patients with severe lymphadenopathy, with a recent history of lymphadenectomy or radiotherapy, or with filariasis).
2. Location and distribution:
1) Local edema: Inflammation, allergy (eg, Quincke edema), impaired venous drainage (eg, deep vein thrombosis [DVT]), impaired lymphatic drainage (eg, malignancy-related lymphadenopathy, erysipelas, filariasis).
2) Generalized edema: Due to cardiac causes (eg, HF), hepatic causes (eg, cirrhosis), renal causes (eg, nephrotic syndrome), endocrine causes (eg, hypothyroidism), malnutrition (eg, protein deficiency, vitamin B1 deficiency), pregnancy; drug-induced (eg, glucocorticoid treatment); idiopathic.
DiagnosisTop
Assess the extent and location of edema (local or generalized).
1. Localized edema: Local inflammatory edema is characterized by pain, warming, and erythema. Edema due to impaired venous drainage is usually asymmetric (except for superior vena cava syndrome) and painless. Clinical examination may reveal features of DVT. Prolonged venous edema leads to trophic changes in the skin. Allergic edema develops rapidly, is pale and painless, and resolves quickly. If venous obstruction is a possibility (based on history and physical examination), compression ultrasonography (CUS) may be used for initial evaluation. If there is a suggestion of obstruction within the pelvis, computed tomography (CT) may be of use.
2. Generalized edema: Significant generalized edema occurs in patients with advanced HF, nephrotic syndrome, or acute or chronic liver disease. These conditions cause major fluid retention and significant weight gain, which may be accompanied by pleural effusion or ascites. In patients who are able to walk, edema usually starts in the lower limbs, while in bedridden patients it affects the sacral area. The edema is usually pitting (applying pressure with a finger produces a pit that disappears slowly). Diagnostic workup depends on the clinical situation.
Generally, history and physical examination are very helpful in differentiating various organ diseases that manifest with generalized edema. Initial laboratory and imaging findings include (if available) attaining a urine dipstick to evaluate for proteinuria, serum albumin level, thyroid-stimulating hormone (TSH) level, and measures of kidney and liver function. Chest radiography, ultrasonography, and echocardiography can also be of use.
Differential diagnosis of generalized edema: Figure 1.13-1.
FiguresTop
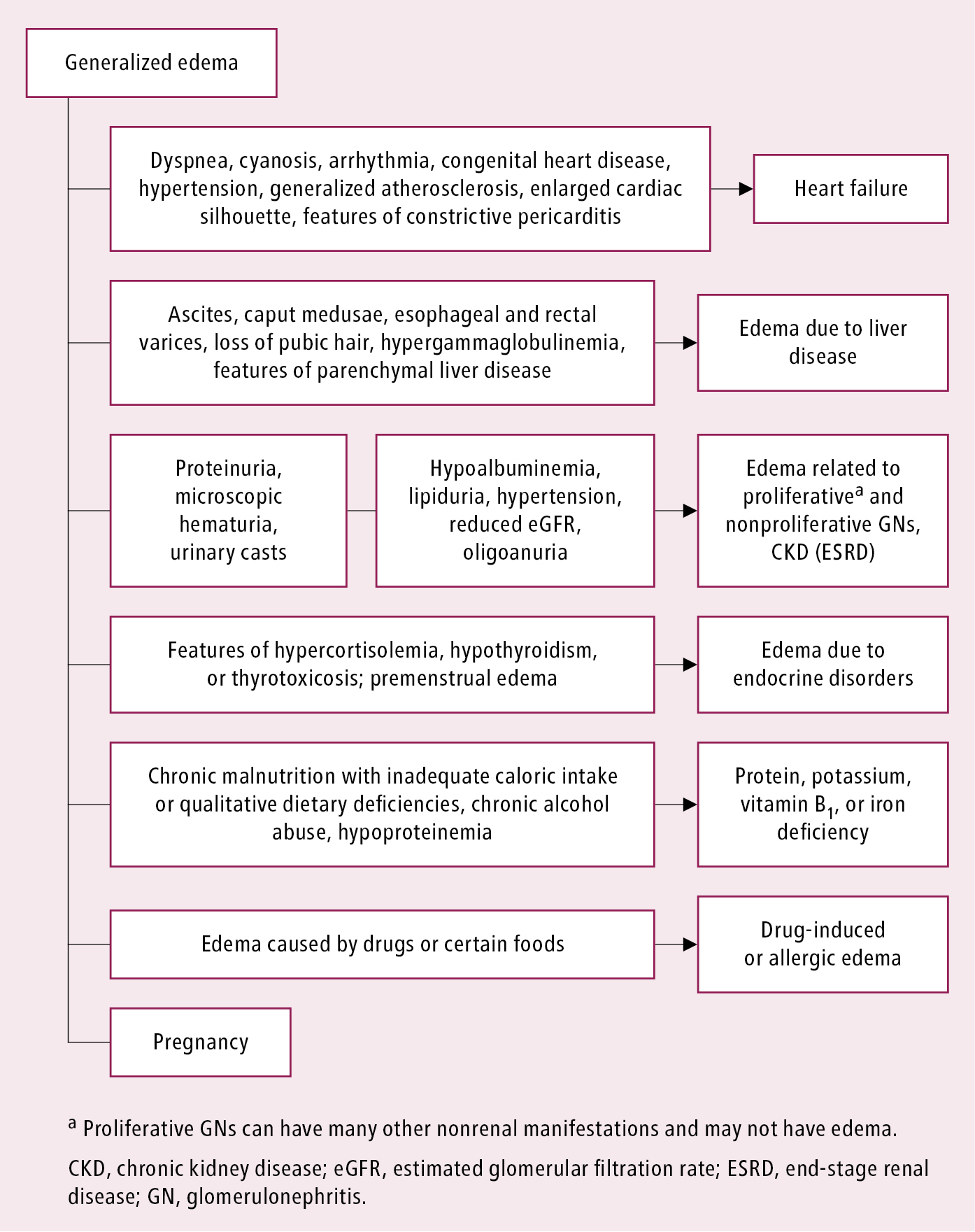
Figure 1.13-1. Differential diagnosis of generalized edema.