 English
English
 Español
Español
 українська
українська

Hyperandrogenism refers to increased levels of serum androgens in women. It can present with hirsutism, oligo- or amenorrhea, acne, androgenic alopecia, and virilization. Although hyperandrogenism can occur in men, it is uncommon and presents with few clinical manifestations. This chapter focuses on the approach to hyperandrogenism in women. Very high androgen levels (ie, serum testosterone >150 ng/dL [5.2 nmol/L]) or dehydroepiandrosterone sulfate (DHEAS) levels >700 microg/dL [18.9 micromol/L]) should increase suspicion for a neoplastic process.
Hirsutism refers to excessive male-pattern hair growth in androgen-dependent areas, such as the upper lip, chest, abdomen, back, buttock, and inner thighs, where women typically have little to no hair. It may be idiopathic, caused by androgen excess, or drug induced.
Virilization occurs with more severe hyperandrogenism and includes deepening of the voice, increased muscle mass, reduced breast and uterus size, abnormal vaginal bleeding, and clitoromegaly, and is often rapid in onset and progressive.
Hypertrichosis refers to generalized excessive hair growth not limited to locations sensitive to androgens and not caused by hyperandrogenism. It may be hereditary, idiopathic, due to acromegaly, or drug induced (phenytoin, penicillamine, diazoxide, minoxidil, cyclosporine [INN ciclosporin]). It may also occur in women with hypothyroidism, anorexia nervosa, porphyria, or dermatomyositis.
Oligomenorrhea is defined as irregular menstrual cycles in women, occurring < 8 times per year or at intervals of >35 days.
Amenorrhea is defined as an absence of menses for ≥3 months in a woman with previously regular menstrual cycles or ≥6 months in any woman with ≥1 previous spontaneous menstruation.
Androgenic alopecia refers to hair loss or thinning of hair in the frontal and crown regions of the scalp.
Causes of androgen excess in women:
1) Ovarian dysfunction: Polycystic ovary syndrome (PCOS) (most common), androgen-secreting ovarian tumor, ovarian hyperthecosis (hyperplasia of the theca interna of the ovary leading to increased production of androgens), luteoma of pregnancy.
2) Adrenal gland dysfunction: Androgen-secreting adrenal tumors, Cushing syndrome, classic and nonclassic congenital adrenal hyperplasia (CAH) caused by 21-hydroxylase or 11beta-hydroxylase deficiency.
3) Other endocrinopathies: Acromegaly, severe insulin resistance syndromes, obesity-induced hyperandrogenic anovulation.
4) Drugs: Androgens, anabolic steroids, danazol, valproic acid, oral contraceptives containing some androgenic progestogens.
5) Idiopathic hirsutism is often due to increased sensitivity to androgens.
Take a history of medications, hirsutism, acne, hair loss/thinning, oligomenorrhea/amenorrhea, galactorrhea, and changes to external genitalia. Symptoms of virilization or symptoms that are abrupt in onset, develop rapidly, or begin post menopause should increase suspicion for an ovarian or adrenal tumor, which may be malignant. Symptoms that first occur in the premenopausal stage or are slower in onset are more typical of benign causes such as PCOS, idiopathic hirsutism, or nonclassic congenital adrenal hyperplasia (NCCAH).
On physical examination, assess the type and distribution of hair in all androgen-sensitive locations, which can indicate the degree of androgen excess. Hirsutism may be assessed with the modified Ferriman-Gallwey score (Figure 1.23-1). The score considers 9 androgen-sensitive areas. The criteria for identifying hirsutism are arbitrary and vary among different ethnic groups, from 2 in Asian to 9 in White and 10 in the Mediterranean populations, although scores much lower than 9 may be associated with androgen excess. Assess for hair loss or thinning in the frontal and crown regions of the scalp to identify androgenic alopecia.
Initial biochemical workup includes total serum testosterone, DHEAS, and 8-am follicular phase (day 1-14) serum 17-hydroxyprogesterone (17-OHP). If the patient has аmеոorrheа or infrequent menses, the sample can be drawn on a random day.
Very high androgen levels, virilization, postmenopausal onset or rapid progression of symptoms are features that warrant urgent pelvic and adrenal imaging (ultrasonography +/- magnetic resonance imaging [MRI]) to assess for an ovarian or adrenal tumor. Pelvic imaging in women with ovarian hyperthecosis typically demonstrates bilateral increase in ovarian stromal volume. Small tumors, especially of an ovarian source, may not be detectable on imaging.
Further tests (seebelow) likely require expert consultation. If imaging is normal. but there is suspicion for a neoplastic process, ovarian and adrenal vein sampling can help identify the source of hyperandrogenism. In postmenopausal women, vein sampling is rarely indicated as it is invasive and does not often change management (bilateral oophorectomy). A less invasive diagnostic tool to help identify ovarian hyperandrogenism is the gonadotropin-releasing hormone (GnRH) agonist stimulation test. In this test, a GnRH agonist (leuprorelin 3.75 mg or triptorelin 3 mg) is administered once, IM or subcutaneously, and serum testosterone is measured at baseline and 4 weeks following the injection. A reduction in testosterone by >50% indicates a luteinizing hormone (LH)–dependent source of hyperandrogenism (ie, more likely hyperthecosis vs ovarian tumor). Of note, virilizing ovarian tumors may not be regulated by gonadotropin and should be suspected in patients without testosterone suppression at 4 weeks post injection and with very high initial testosterone levels.
If there is evidence of severe insulin resistance in the setting of androgen excess, further workup including fasting serum insulin, glycated hemoglobin (HbA1c), oral glucose tolerance test (OGTT), C-peptide, and possibly genetic testing is recommended to assess for syndromes of severe insulin resistance.
In patients with gradual onset of symptoms or biochemical markers that are normal or only mildly elevated, consider PCOS, Cushing syndrome (although certain causes of Cushing syndrome could be more rapid), NCCAH, or idiopathic hirsutism. Additional biochemical workup includes follicle stimulating hormone (FSH), LH, estradiol, androstenedione and sex hormone-binding globulin (SHBG) measurements.
Assess for PCOS using the Rotterdam criteria (diagnosed if 2 out of the 3 criteria are met: irregular menstrual cycles, oligomenorrhea, amenorrhea, anovulation; clinical or biochemical hyperandrogenism; and polycystic ovarian morphology on pelvic ultrasound imaging; after other causes have been excluded).
Consider a 1-mg overnight dexamethasone suppression test to assess for cortisol suppression and 24-h urine free cortisol or late-night salivary cortisol if there are features suggestive of Cushing syndrome.
If 17-OHP levels are significantly elevated (>6 nmol/L [>200 ng/dL]), assess for NCCAH with a 250-microg ACTH stimulation test. A serum 17-OHP level >1500 ng/dL (43 nmol/L) after ACTH stimulation confirms the diagnosis. If the results are within the range between 1000 ng/dL (30 nmol/L) and 1500 ng/dL (43 nmol/L), the diagnosis should be confirmed with genotyping of the СΥP21A2 gene. Classic adrenal hyperplasia is typically diagnosed at birth through newborn testing.
Differential diagnosis of hyperandrogenism: Table 1.23-1. Diagnostic algorithm for hyperandrogenism and hirsutism: Figure 1.23-2.
Assess the impact of hirsutism and hyperandrogenism on the patient and whether treatment is desired, and treat the underlying cause if possible. Discontinue any potentially responsible medications.
First-line pharmacologic therapy for hyperandrogenism and hirsutism in premenopausal women with PCOS or idiopathic hirsutism is an estrogen-progestin contraceptive or spironolactone (antiandrogen) if there are no contraindications. If contraceptives are contraindicated or response to this therapy is not adequate after 6 months, spironolactone may be considered as monotherapy or in combination therapy. Patients should be counseled on the teratogenic effects of spironolactone in pregnancy and the need for adequate contraception. In postmenopausal women, spironolactone is the recommended therapy over contraceptives.
If the patient has PCOS, assess for associated conditions, such as metabolic risk factors (obesity, impaired glucose tolerance [IGT], diabetes mellitus, dyslipidemia), obstructive sleep apnea (OSA), and anovulatory infertility. Counsel on lifestyle changes including diet and weight loss, as this may decrease insulin resistance, lower serum androgen levels/hirsutism, improve fertility rate, and reduce anovulation/menstrual irregularity. Consider metformin in patients with obesity, diabetes, and IGT or impaired fasting blood glucose (IFG). Glucagon like peptide-1 (GLP-1) receptor agonists can be considered for obesity as per the general population guidelines. Patients with oligomenorrhea are at an increased risk for endometrial hyperplasia and endometrial malignancy. Combined estrogen-progestin contraceptives are the first-line therapy for menstrual dysfunction, endometrial protection, and for hirsutism. If combined contraceptives are contraindicated or there is no need for contraception, endometrial protection can be achieved using progestin-containing methods, including progestin-only pills, a progestin-releasing intrauterine device, or cyclic progestin therapy to induce withdrawal bleeding. Referral to specialists (eg, endocrinologists, gynecologists, infertility specialists) may be needed.
Referral for surgery is indicated for Cushing syndrome (most cases), ovarian tumors, ovarian hyperthecosis, or adrenal tumors. GnRH therapy can be offered to patients with hyperandrogenism of an ovarian source who are not surgical candidates, especially for ovarian hyperthecosis.
Consider direct hair removal methods (waxing, shaving, electrolysis, laser) for mild hirsutism with no underlying endocrinopathies. Eflornithine is a topical pharmacologic option for temporary facial hair removal.
Given the potential psychologic impact of hirsutism and hyperandrogenism on women, provide mental health screening and therapy as indicated.
TABLES AND FiguresTop
|
Endocrinopathy |
Timing of onset/diagnosis |
Expected results of investigations |
| Frequent |
|
|
|
PCOS |
Ages 15-25 (peripubertal onset) |
Rotterdam criteria (2+ of 3 needed): – Clinical or biochemical hyperandrogenism – Irregular menstrual cycles (oligomenorrhea/amenorrhea/anovulation) – Polycystic ovaries (transvaginal/pelvic US) and excluded other causes |
|
Idiopathic hirsutism |
Ages 15-25 (peripubertal onset) |
Normal androgen levels, diagnosis of exclusion |
|
Infrequent |
|
|
|
NCCAH |
Adolescence/peripubertal onset or early adulthood (more common in certain ethnic groups) |
– Morning serum 17-OHP >200 ng/d (>6 nmol/L) – Serum 17-OHP >1500 ng/dL (43 nmol/L) following a 250-microg ACTH stimulation test |
|
Classic 21-hydroxylase deficiency |
Congenital |
Very high neonatal 17-OHP (3500-5000 ng/dL [105-150 nmol/L]) on a heel-stick blood spot |
|
Ovarian hyperthecosis |
Onset in the third decade or later (usually postmenopausal) |
– Very high testosterone levels (>5.2 nmol/L [>150 ng/dL]) – Suppression of testosterone after gonadotropin-releasing hormone stimulation test – Diagnosis may be supported radiographically +/- histologic assessment of ovaries |
|
Drugs |
Not applicable |
Not applicable |
|
Rare |
|
|
|
Severe insulin resistance syndromes |
Adolescence or adulthood |
– Fasting serum insulin >150 pmol/L (21.6 microU/mL) and/or a peak insulin >1500 pmol/L (216 microU/mL) during OGTT – Significantly elevated serum testosterone leves (>5.2 nmol/L [>150ng/dL]) |
|
Androgen-secreting ovarian tumors |
Onset in the third decade or later (usually postmenopausal) |
– Very high testosterone levels (>5.2 nmol/L [>150 ng/dL]) – Unlikely to see suppression of testosterone after gonadotropin-releasing hormone stimulation test – May be visible on ovarian imaging (US/MRI) |
|
Androgen-secreting adrenal tumors |
Variable, but adrenal cancer peaks <5 years of age and in the fourth and fifth decades of life |
– Very high DHEAS levels (>700 microg/dL [18.9 micromol/L]) – Usually visible on non–contrast enhanced adrenal CT |
|
Cushing syndrome |
Variable, depending on cause |
– Morning cortisol >1.8 microg/dL (50 nmol/L) after a 1-mg dexamethasone suppression test – High 24-h urine free cortisol or late-night salivary cortisol |
|
Acromegaly |
Variable, but usually 40-45 years of age |
– Elevated serum insulin growth-like factor 1 – Growth hormone concentration >1 ng/mL 2 h after a 75-mg OGTT |
|
Gestational hyperandrogenism |
During pregnancy |
Elevated testosterone and/or DHEAS beyond normal range for pregnancy |
| 17-OHP, 17-hydroxyprogesterone; ACTH, adrenocorticotropic hormone; CT, computed tomography; DHEAS, dehydroepiandrosterone sulfate; MRI, magnetic resonance imaging; NCCAH, nonclassic 21-hydroxylase deficiency; OGTT, oral glucose tolerance test; PCOS, polycystic ovary syndrome; US, ultrasonography. | ||
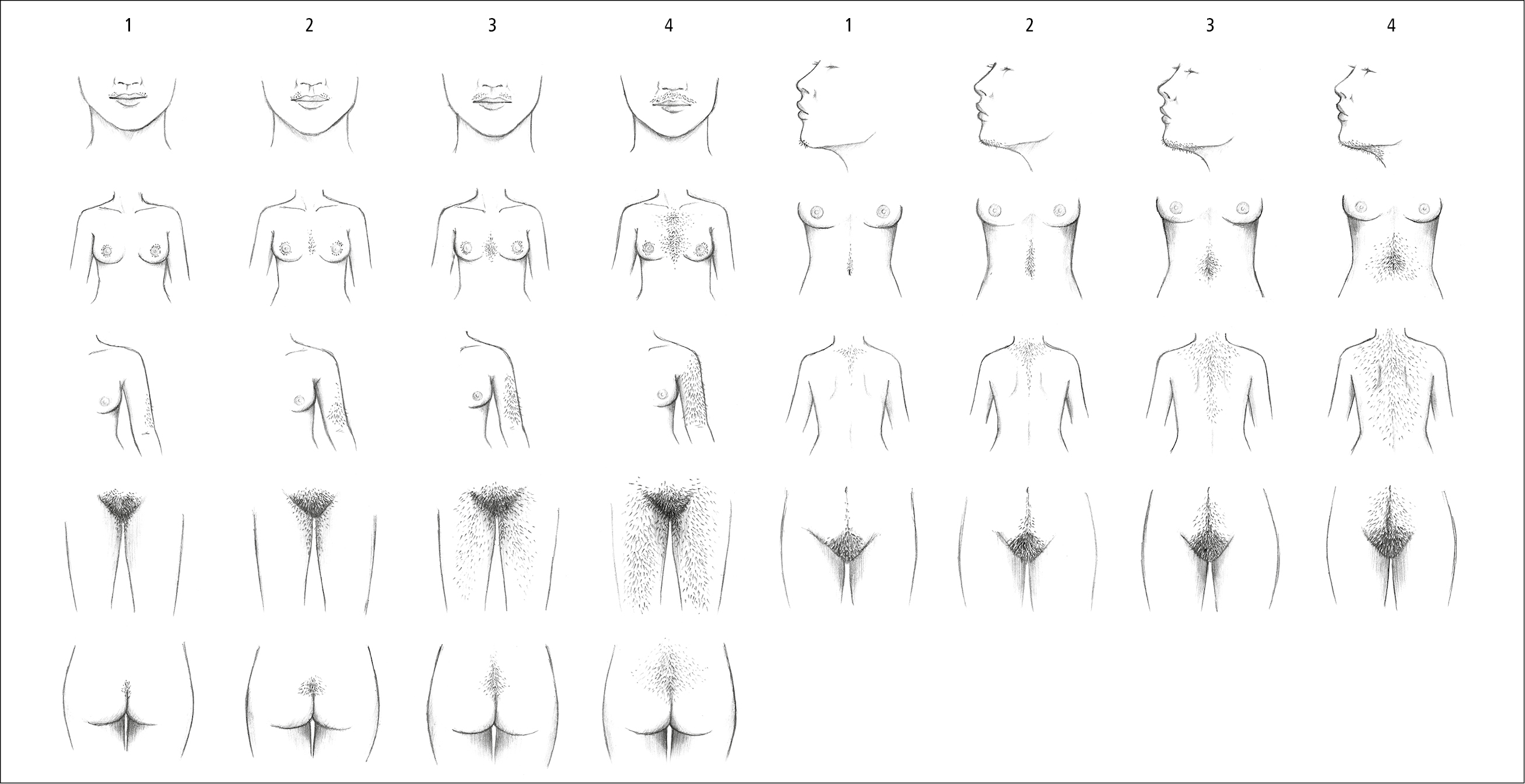
Figure 1.23-1. Ferriman-Gallwey score. Illustration courtesy of Dr Shannon Zhang.
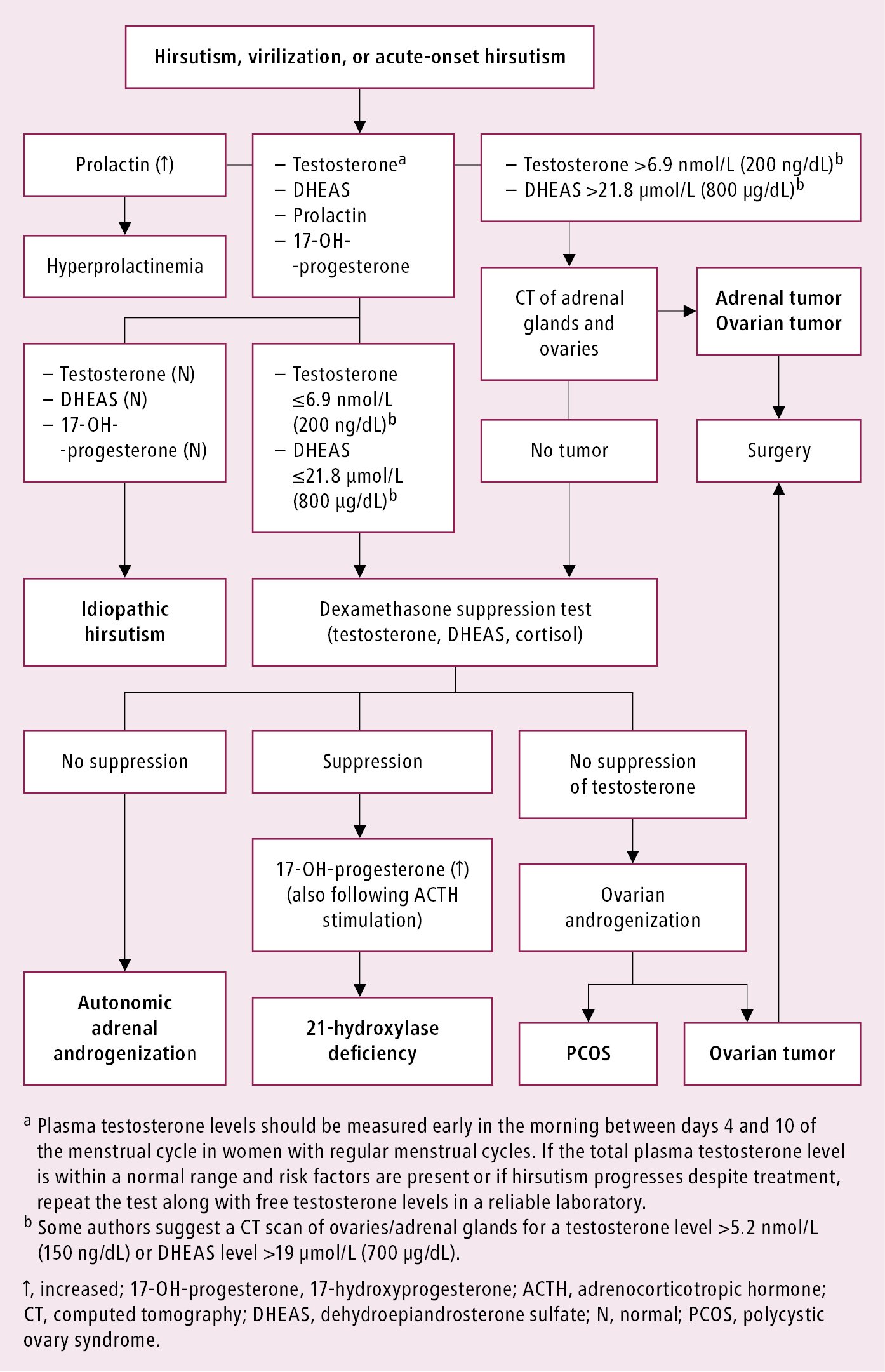
Figure 1.23-2. Diagnostic algorithm for hirsutism and virilization.