 English
English
 Español
Español
 українська
українська

Vahanian A, Beyersdorf F, Praz F, et al; ESC/EACTS Scientific Document Group. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022 Feb 12;43(7):561-632. doi: 10.1093/eurheartj/ehab395. Erratum in: Eur Heart J. 2022 Feb 18;: PMID: 34453165.
Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021 Feb 2;143(5):e35-e71. doi: 10.1161/CIR.0000000000000932. Epub 2020 Dec 17. Erratum in: Circulation. 2021 Feb 2;143(5):e228. Erratum in: Circulation. 2021 Mar 9;143(10):e784. PMID: 33332149.
Definition, Etiology, PathogenesisTop
Tricuspid stenosis (TS) is a reduction of the tricuspid valve orifice area, which causes impaired right ventricular filling.
Etiology: Rheumatic fever; other, very rare etiologies include carcinoid syndrome. Right atrial myxoma or other tumors of the right atrium, tricuspid valve vegetations, and right atrial thrombus can cause tricuspid inflow stenosis not related to the valve but with similar physiologic consequences. Tricuspid atresia is a rare congenital anomaly affecting the tricuspid valve with other associated lesions. Patients with previous tricuspid valve replacement can develop prosthetic valve stenosis. The majority of patients have mixed TS and tricuspid regurgitation (TR), such as those with carcinoid syndrome.
Clinical FeaturesTop
1. Symptoms: Progressive fatigue, loss of appetite, mild dyspnea. Palpitations related to atrial arrhythmias are common.
2. Signs: A tricuspid opening snap, presystolic murmur (in sinus rhythm), an early- and mid-diastolic murmur (rarely holodiastolic), most prominent during inspiration; signs of right ventricular failure (see Chronic Heart Failure), pulsations of the liver (presystolic pulsation is typical).
DiagnosisTop
1. Electrocardiography (ECG): P pulmonale; frequently atrial fibrillation or atrial flutter. There may be features of enlargement of both atria (due to the frequent coexisting mitral valve disease in patients with rheumatic heart disease). The amplitude of the QRS complex may be low in V1 due to right atrial enlargement.
2. Chest radiography: Right atrial enlargement and dilation of the superior vena cava. Pulmonary perfusion may be reduced.
3. Echocardiography (Figure 3.18-12): Evaluation of the valve morphology and severity of the defect. A mean transvalvular gradient of ≥5 mm Hg at a normal heart rate is considered indicative of clinically significant TS. Given the association with rheumatic heart disease, the left-sided valve should be fully assessed. In cases of suspected carcinoid syndrome, there is often pulmonary valve involvement with combined stenosis and regurgitation.
TreatmentTop
1. Medical treatment: Diuretics (agents: see Table 3.9-4) and fluid and sodium restriction.
2. Invasive treatment should be considered in patients with severe TS who are (1) symptomatic; or (2) undergoing intervention on left heart valves (percutaneous valvotomy may be attempted in patients eligible for percutaneous mitral commissurotomy). In patients with isolated severe TS, consider percutaneous tricuspid balloon valvotomy; in patients with coexisting mitral valve disease, surgical treatment is indicated. Valve morphology can provide clues as to the underlying etiology.
FiguresTop
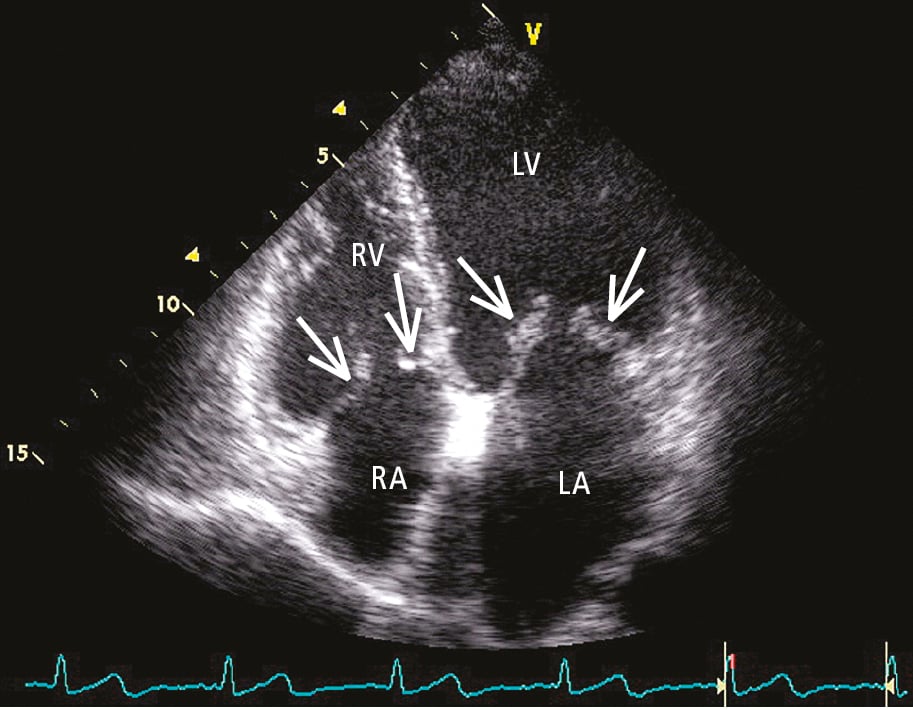
Figure 3.18-12. Transthoracic echocardiography (TTE; apical 4-chamber view): mitral valve disease with tricuspid valve stenosis. Organic lesions of the leaflets with reduced leaflet opening (arrows). LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle.